- Main idea: Clinical reasoning is a repeatable thinking loop that turns scattered clues into safe priorities, clear actions, and checked results.
- The cycle: Work through 8 phases from situation and cue collection to processing, problem picking, goal setting, action, outcome evaluation, and reflection, then loop back when new info changes the picture.
- What separates pros from novices: Experienced clinicians assess in a consistent pattern, resist confirmation bias, consider multiple causes before locking in, and prioritize life threats first.
- Interview signal: Hiring panels care less about a perfect guess and more about hearing your logic, your priorities, and how you recheck whether your plan actually worked.
- How to show it fast: In scenarios, state your first impression, walk the steps out loud, set measurable goals, mention reassessment timing, and explain how you would pivot if outcomes do not improve.
Thinking Like a Healthcare Professional
The clinical reasoning cycle transforms scattered observations into systematic patient care. Novice clinicians collect information randomly and jump to conclusions. Experienced professionals follow structured processes that ensure nothing critical gets missed, prioritize appropriately, and evaluate whether interventions achieve intended outcomes.
Mastering the clinical judgment process matters because healthcare interviews assess not just what you know, but how you think. When presented with patient scenarios, interviewers evaluate whether you approach problems systematically, consider multiple possibilities, recognize when to escalate, and circle back to verify your interventions worked.
This guide breaks down the complete cycle from initial assessment through final evaluation, showing how expert clinicians think through complex patient situations.
The Eight-Phase Clinical Reasoning Cycle
The clinical reasoning cycle provides a systematic framework for processing patient information and making sound decisions. Each phase builds on the previous, creating a continuous loop of assessment, intervention, and evaluation.
| Phase | Key Question | Primary Activity |
|---|---|---|
| 1. Consider the Patient Situation | What’s happening here? | Initial impression, context gathering |
| 2. Collect Cues/Information | What data do I need? | Systematic assessment, vital signs, history |
| 3. Process Information | What does this mean? | Interpret findings, identify patterns |
| 4. Identify Problems/Issues | What’s wrong? | Formulate diagnoses or concerns |
| 5. Establish Goals | What should happen? | Define desired patient outcomes |
| 6. Take Action | What will I do? | Implement interventions |
| 7. Evaluate Outcomes | Did it work? | Reassess patient status |
| 8. Reflect on Process | What did I learn? | Consider what worked and what didn’t |
💡 Pro tip: This cycle isn’t always linear. You often loop back – new information during evaluation might reveal you misidentified the problem, requiring reassessment and revised interventions.
Phase 1: Consider the Patient Situation
Before diving into detailed assessment, experienced clinicians pause to consider context. What’s the overall picture? Is this emergency or routine? What do I already know about this patient? What might be relevant from their history, diagnosis, or current treatments?

Forming Initial Impressions
Your initial impression guides what you assess first. A patient clutching their chest gets immediate cardiac evaluation. Someone confused and disoriented prompts neurological and metabolic assessment. This contextual awareness prevents getting lost in details while missing urgent issues.
- 🎯 Chief complaint: Why is the patient here now?
- 📋 Relevant history: Chronic conditions, recent procedures, current medications
- ⚡ Acuity level: Stable, concerning, or emergent?
- 🔍 Environmental context: Home, clinic, hospital, emergency department?
Expert advice: In interviews, when given patient scenarios, pause briefly to state your initial impression before diving into specifics. “This sounds like a potential respiratory emergency, so I’d first ensure airway is patent.” This demonstrates you’re thinking systematically, not just reacting.
Phase 2: Collect Cues and Information
Systematic patient assessment prevents missing critical information. Novices collect data randomly. Experts follow structured approaches that ensure comprehensive evaluation while prioritizing urgent findings.
Types of Assessment Data
Complete assessment combines subjective information (what patient reports) with objective findings (what you measure or observe). Both matter – patients’ subjective experience guides your objective examination focus.
| Data Type | Sources | Examples |
|---|---|---|
| Subjective | Patient report, family input | Pain description, symptom history, concerns |
| Objective | Vital signs, physical exam, labs | BP 160/95, diminished breath sounds, Na+ 128 |
| Historical | Medical records, prior visits | Chronic conditions, allergies, past surgeries |
| Contextual | Social situation, resources | Living alone, medication access, support system |
Systematic Assessment Approaches
Use structured frameworks to ensure comprehensive assessment. Head-to-toe, body systems review, or focused assessments depending on situation. The key is consistency – following the same pattern every time prevents omissions.
- ABCs first: Always assess Airway, Breathing, Circulation in emergent situations
- Vital signs baseline: Obtain complete vital signs unless emergency requires immediate intervention
- Focused then comprehensive: Address urgent concerns first, then broaden assessment
- Use validated tools: Pain scales, fall risk assessments, depression screens
- Document as you go: Don’t rely on memory for detailed findings
Never skip assessment steps because you think you know what’s wrong. Confirmation bias causes errors. Collect data systematically before jumping to conclusions.
Phase 3: Process Information
Raw data becomes meaningful through interpretation. This phase requires integrating findings, recognizing patterns, and considering multiple possible explanations. Expert clinicians don’t just collect information – they analyze what it means in context.
Pattern Recognition and Clustering
Group related findings together. Fever, elevated white count, and localized pain cluster into infection pattern. Multiple bruises, low platelet count, and bleeding gums suggest coagulation problem. Pattern recognition accelerates diagnosis but requires guarding against premature closure.
- 🔗 Cluster related findings: Which symptoms and signs go together?
- ⚖️ Compare to normals: Is this finding expected for this patient?
- 📊 Consider trends: Are things improving, stable, or worsening?
- 🧩 Look for outliers: What doesn’t fit the obvious pattern?
Expert advice: When processing information in interviews, verbalize your thinking: “The tachycardia, hypotension, and decreased urine output together suggest hypovolemia.” This demonstrates nursing process steps of synthesizing data rather than just listing findings.
Considering Multiple Possibilities
Generate multiple working hypotheses before committing to one diagnosis. What else could explain these findings? This prevents anchoring on the first explanation that comes to mind and missing serious but less obvious conditions.
💡 Pro tip: Use the mnemonic VINDICATE (Vascular, Inflammatory, Neoplastic, Degenerative, Intoxication, Congenital, Autoimmune, Trauma, Endocrine) to systematically consider diagnostic categories.
Phase 4: Identify Problems and Issues
Transform your analysis into clear problem statements or nursing diagnoses. Good problem identification is specific, prioritized, and actionable. Vague problems lead to vague interventions.
Prioritizing Multiple Problems
Patients rarely present with single isolated problems. You must prioritize which issues need immediate attention versus which can wait. Life-threatening problems always come first, followed by those causing significant distress or risking serious complications.
| Priority Level | Criteria | Examples |
|---|---|---|
| Immediate (Priority 1) | Life-threatening, requires instant action | Airway obstruction, severe bleeding, chest pain |
| Urgent (Priority 2) | Could become life-threatening if delayed | Acute pain, high fever, significant anxiety |
| Important (Priority 3) | Needs attention but not emergent | Medication teaching, wound care, mobility issues |
| Routine (Priority 4) | Can be scheduled, important for long-term outcomes | Preventive care, health promotion, routine monitoring |
Writing Effective Problem Statements
Problem statements should be specific enough to guide interventions. “Patient uncomfortable” doesn’t direct action. “Acute pain rated 8/10 in surgical incision site, limiting mobility” clearly identifies what needs addressing and how you’ll measure improvement.
- Use standardized language when appropriate (NANDA nursing diagnoses, medical diagnoses)
- Include contributing factors when known (“Impaired gas exchange related to pneumonia”)
- Make problems measurable so you can evaluate whether interventions work
- Update problem lists as situations evolve
Phase 5: Establish Goals
Clear goals guide intervention selection and provide benchmarks for evaluation. Goals should be specific, measurable, achievable, relevant, and time-bound (SMART). Vague goals like “patient will feel better” don’t tell you what to do or when you’ve succeeded.
Short-Term vs Long-Term Goals
Distinguish between immediate targets and broader outcomes. Short-term goals address acute issues within hours or days. Long-term goals focus on ultimate desired outcomes, which may take weeks or months.
- ⚡ Short-term example: Pain reduced to 3/10 or less within 30 minutes of medication
- 📈 Long-term example: Patient demonstrates independent ambulation with walker before discharge
- 🎯 Intermediate example: Patient correctly demonstrates wound care procedure by end of shift
💡 Pro tip: In interviews, when discussing patient scenarios, state your goals explicitly: “My immediate goal is stabilizing vital signs, then I’d work toward pain management and patient education.” This shows you’re thinking systematically about desired outcomes.
Patient-Centered Goal Setting
Goals should reflect patient priorities, not just clinical targets. A patient’s goal might be “attend grandson’s graduation next month” while your clinical goal is “improve functional capacity.” Both matter, but the patient’s goal provides motivation and meaning.
Expert advice: Involve patients in goal-setting whenever possible. “What’s most important to you right now?” Their answers guide which clinical goals to prioritize when multiple issues compete for attention.
Phase 6: Take Action
Implementation translates plans into concrete interventions. This includes both independent actions within your scope and collaborative interventions requiring physician orders or interdisciplinary coordination.
Categories of Nursing Interventions
Healthcare interventions span multiple domains. Effective care requires balancing all categories, not just focusing on physical tasks.
| Intervention Type | Description | Examples |
|---|---|---|
| Independent | Within your scope, no order needed | Positioning, patient teaching, comfort measures |
| Dependent | Requires physician order | Medication administration, lab draws, procedures |
| Collaborative | Interdisciplinary coordination | Care conferences, discharge planning, referrals |
| Preventive | Reduce risk of complications | Fall prevention, skin care, infection control |
| Educational | Increase knowledge/skills | Disease teaching, medication instruction, self-care |
Safe Implementation Practices
Taking action requires constant vigilance for safety. Verify orders, confirm patient identity, assess for contraindications before proceeding. Never skip safety steps because you’re rushed or the patient is familiar.
- Follow the “5 Rights”: Right patient, medication, dose, route, time
- Verify orders against what seems appropriate for patient condition
- Question anything that doesn’t make clinical sense
- Document immediately after interventions, include patient response
- Communicate changes to relevant team members
If an intervention doesn’t feel right, pause and verify. Trusting your instinct that something’s off prevents errors more often than blindly following orders.
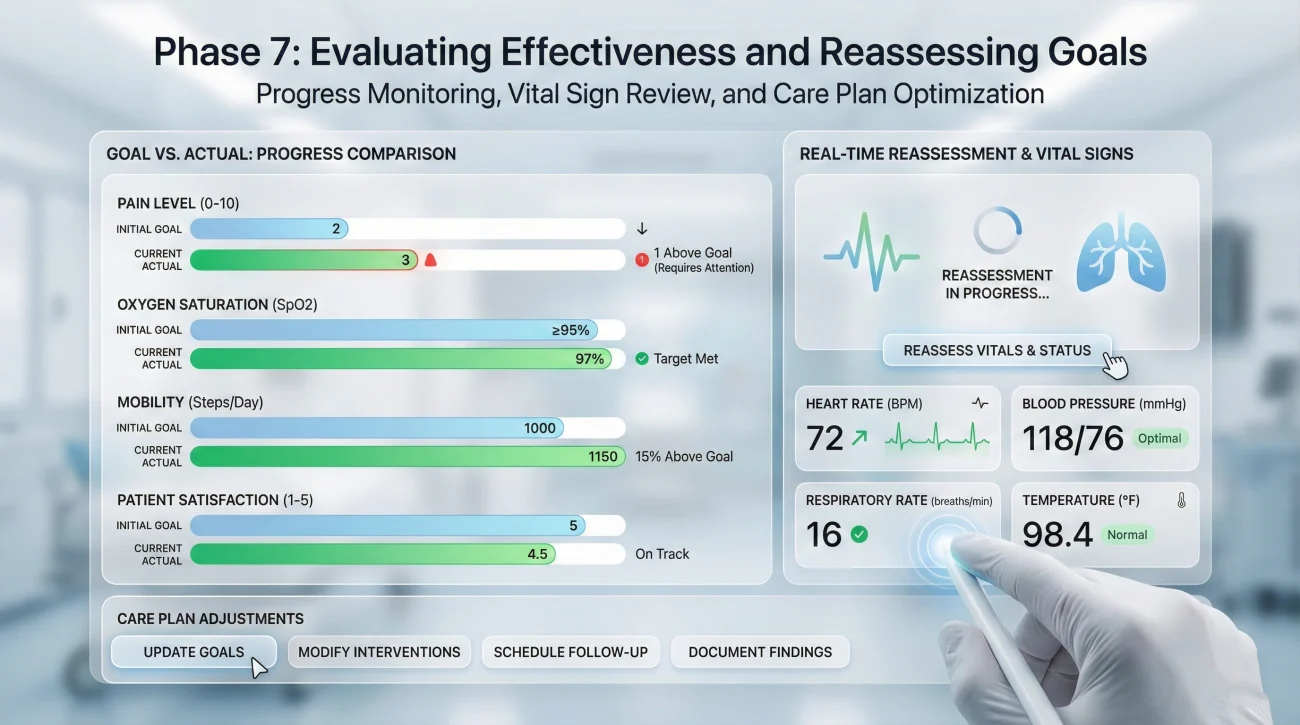
Phase 7: Evaluate Outcomes
Evaluation closes the loop by reassessing whether interventions achieved intended goals. This isn’t optional – it’s how you know if your clinical reasoning was sound and your interventions effective.
When to Reassess
Timing matters. Some interventions require immediate reassessment (did pain medication work within 30 minutes?), while others need longer timeframes (is physical therapy improving mobility over days?). Build reassessment into your workflow systematically.
- ⏱️ Immediate: After urgent interventions, verify improvement
- 📅 Short-term: Check medication effectiveness, acute symptom changes
- 📆 Long-term: Monitor progress toward discharge goals, functional improvements
- 🔄 Continuous: Ongoing monitoring of vital patients, unstable conditions
Analyzing Outcomes
Compare current status to established goals. Did you achieve what you intended? If yes, continue current plan. If no, determine why – was the diagnosis wrong? Intervention inappropriate? Goals unrealistic? This analysis guides your next cycle of reasoning.
Expert advice: In interview scenarios, always circle back to evaluation: “After implementing these interventions, I’d reassess vital signs and pain level to determine effectiveness.” Failing to mention evaluation signals incomplete medical decision making process.
Don’t assume interventions worked without verification. Patients sometimes say they’re “fine” to avoid bothering you, even when they’re still suffering.
Phase 8: Reflect on Process and Learning
Reflection transforms experience into expertise. What worked? What didn’t? What would you do differently next time? This metacognitive step separates clinicians who plateau after a few years from those who continue developing advanced judgment.

Structured Reflection Questions
Use consistent questions to guide reflection after complex or challenging situations:
- What was most effective about my approach?
- What would I do differently if faced with similar situation?
- What additional knowledge or skills do I need?
- What assumptions did I make that might have been wrong?
- Who could I have consulted earlier or more effectively?
💡 Pro tip: Keep a brief reflection journal for challenging cases. Over time, you’ll recognize patterns in your clinical reasoning strengths and areas needing development.
Demonstrating Clinical Reasoning in Interviews
Healthcare interviews assess clinical reasoning through hypothetical scenarios and questions about past experiences. Strong candidates verbalize their thinking process, showing systematic approach rather than jumping to conclusions.
Walking Through Scenarios Systematically
When given patient scenarios, resist the urge to immediately state a diagnosis. Instead, walk through the cycle: “I’d start by considering the overall situation… then I’d systematically assess… these findings together suggest… my priority problems would be… and I’d establish these goals…”
This structured approach demonstrates expert thinking even if your specific diagnosis isn’t perfect. Interviewers care more about your reasoning process than whether you guessed correctly.
Showing Adaptive Reasoning
Strong answers acknowledge when you’d need to loop back. “If these interventions don’t improve symptoms within the expected timeframe, I’d reassess whether I identified the correct problem and consider alternative explanations.” This shows you understand clinical reasoning is iterative, not linear.
For comprehensive strategies on structuring interview responses and demonstrating clinical competence, explore interview preparation resources for healthcare professionals.
❓ FAQ
🎯 How do I develop clinical reasoning skills as a new graduate?
Practice verbalizing your thinking process with preceptors and experienced colleagues. After patient encounters, walk through the cycle explicitly: what data did I collect, how did I interpret it, what problems did I identify, etc. Reflection after both successful and unsuccessful outcomes accelerates learning.
💼 What if I realize mid-way through that my initial assessment was wrong?
Revise your thinking immediately. Don’t continue with interventions based on incorrect assessment just to avoid admitting error. Acknowledge the new information, reassess systematically, and adjust your plan. Flexibility and willingness to reconsider demonstrates strong clinical reasoning cycle skills, not weakness.
⏰ How do I maintain systematic thinking when overwhelmed with multiple critical patients?
Use the cycle in abbreviated form. Quick mental checklist: situation, key cues, immediate problem, urgent goal, action. Even 10 seconds of structured thinking prevents critical omissions. Triage forces you to prioritize, but don’t skip the thinking framework entirely.
📋 Should I document my entire clinical reasoning process?
Document key elements: relevant assessment findings, identified problems, goals, interventions, and evaluation of effectiveness. You don’t need to document every step of your internal reasoning, but records should show systematic approach and rationale for decisions made.
✨ How detailed should my problem identification be in emergencies?
In true emergencies, you act first based on immediate life threats (ABCs), then refine problem identification as situation stabilizes. The cycle still applies but accelerates. Mental note: “Respiratory distress, need oxygen now, will assess cause during intervention.” Detailed analysis follows once patient is stable.
Final Thoughts
Mastering the clinical reasoning cycle transforms intuitive reactions into systematic professional judgment. This eight-phase framework – from considering initial patient situation through reflecting on outcomes – provides the structure expert clinicians use to process complex information, prioritize competing demands, and evaluate whether their interventions actually work.
Strong clinical reasoning doesn’t mean having all the answers instantly. It means thinking systematically, considering multiple possibilities before committing to one, establishing clear measurable goals, and circling back to verify your interventions achieved intended outcomes. This iterative process, repeated thousands of times across your career, builds the pattern recognition and judgment that defines expertise.
Healthcare interviews assess this reasoning process because it predicts real-world performance better than knowledge alone. Demonstrate through your scenario responses and past experience stories that you approach patient care systematically, recognize when to loop back and reassess, and continuously learn from outcomes both successful and disappointing. That’s what separates novice thinking from expert clinical judgment.
⚠️ Disclaimer: The interview strategies, sample answers, and negotiation tips provided in this guide are for educational purposes only. Hiring decisions are subjective and vary by company and industry. While these strategies are based on professional HR standards, they do not guarantee a specific job offer or result.